 English
English Turkish
Turkish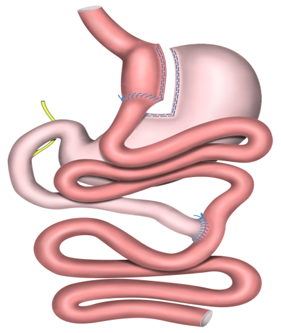
Roux-N-Y Gastric Bypass
Roux-en-Y Gastric Bypass is the most common obesity surgery operation worldwide, mainly USA. Roux-en-Y Gastric Bypass is both stomach reducing and absorption restricting operation. Amount of meal that you eat decreases and it also provides discharge of some foods without absorption.
Like all obesity operations, Roux-en-Y Gastric Bypass operation is applied for fat patients who can not loose weight by diet and exercise. Roux-en-Y Gastric Bypass provides you to loose weight that you ca not loose with diets and heavy exercises without struggling within a short period.
Am I Eligible for Roux-en-Y Gastric Bypass?
Roux-en-Y Gastric Bypass is performed due to same indications with all other obesity surgery metahods. Eligibility of patients for obesity surgery is determined according to consensus decisions which have been published by Nationa Institutes of Health(NIH) in 1991:
- Morbidly obese patients with body mass index > 40 kg/m2,
- Patients with class ll obesity with body mass index > 35 kg/m2 who have diabetes, hypertension, sleep-apnea, heart disease, polycystic ovary syndrome etc. due to obesity,
- If your body mass index is over 35 kg/m2 and you can not loose against any kind of diets or exercises, obesity surgery is the most perfect choice for you.
How is Roux-N-Y Gastric Bypass Operation Performed?
Roux-N-Y Gastric Bypass Operation is performed laparoscopically. In other words, no big cuts are applied on the abdomen. It is performed by using specific tools and cameras through 6 cuts of which all are below 1 cm.
1. First, a small stomach is created on gastric orifice. This is called gastric pouch. Volume of the gastric pouch which is created new is less than a small tea glass. In other words, the volume is about 35 to 50 cc. If your normal gastric volume is between 800 and 1000 cc, your gastric volume is reduced over 95% in this case.
2. A new tract is required to provide food passage into the intestines for this gastric pouch created. For this, your small intestines are cut from 50 to 75 cm. The end going downwards is taken up and connected to the new gastric pouch. So, foods eaten come to the new gastric pouch. The previous stomach stays passive and never meets with food. Foods coming to the new gastric pouch pass into the small intestine which is directly connected. So, remaining stomach and some small intestine part are separated from food passage not to contact with food anymore. This procedure prevents complete absorption of foods and increase strength of weight loss.
3. Stomach separated from food passage and small intestines continuing should transmit their secretion into the remaining small intestine somehow. This is necessary for absorption of foods and some minerals that we need for a healthy life and it is essential that if this connection is not performed, problems may arise. So, the initial part of small intestine where no food passage exists only functions as a transmission channel for bile and pancreas secretion. We connect ends of this small intestine onto a point on the middle of the small intestine connected to the new stomach.
So, your small stomach created by Roux-en-Y Gastric Bypass operation allows to eat in less portions. This less meal is sufficient for you to provide a well fullness feeling. Skipping initial part of small intestines prevents absorption of all foods in the meals that you eat. So, high calories especially taken with fats and bakery products are discharged from intestines without absorption.
You loose weight fast and efficiently without struggling with Roux-en-Y Gastric Bypass. This fast weight loss process decreases when you reach to your normal weights and stops completely after 2 years. Some weight gain may occur in about 35% of patients after 5 years. This is the most robust indicator that the operation does not cause uncontrolled weight loss.
What are mechanisms of Action of Roux-N-Y Gastric Bypass Operation?
A Small Gastric Pouch: Gastric volume is reduced by 90 to 95% with Roux-N-Gastric Bypass operation. A normal human stomach may stretch up to 1000 cc volume. This capacity may increase to 1500 cc volume when obesity increases. The new gastric pouch created with Roux-en-Y Gastric Bypass operation is about 35 to 50 cc. A stomach reduced this much may intake very restricted amount of food. When gastric lumen is full with food and starts to stretch, it sends a stimulus to satiety center and provides feeling of fullness sense. Thus, fullness sense starts with the first bite.
Hormonal Effect: Foods passing from small gastric pouch into small intestine cause secretion of different hormones from small intestine. These hormones secreted from small intestine are generally called incretins. These hormones called incretins (Cholecystokinin, Peptide-YY, GLP-1) which are stimulated by entering of foods into the small intestine provide sense of fullness. This sense of fullness created by incretins also affect use of simple sugar (glucose) absorbed positively. Especially GLP-1 hormone increases much when foods reach to ileum, last part of small intestine reduces blood glucose of patients with diabetes to normal levels without drugs. Intraabdominal lipoidosis increased in obesity cause increase of resistin hormone. Resistin is a hormone which creates resistance on fat tissues against effect of insulin hormone. Intraabdominal fat tissue decreases with Roux-N-Y Gastric Bypass. Production of resistin hormone regresses to normal levels. Insulin resistance decreases. The insulin resistance decreases accelerated weight loss.
Metabolic Effect: Metabolism is sum of all activities that our body does for life. Some of these are voluntary actions and behaviors. For example, eating, drinking water, moving etc. Large part of our metabolism consists of works done by all tissues from our organs to our cells individually involuntarily. Heart beating, operation of brain, stomach and intestines, hormone secretion, clearance of blood in liver and kidney from toxic wastes. So, our metabolism continue to work and consume energy while we are at sleep or resting. Our energy need decreases during resting status, but we need energy for all these basic activities. This energy is provided from glucose and fat deposits when we eat.
The energy consumption during resting status increases in patients who have Roux-N-Y Gastric Bypass operation. The underlying mechanism of increase in basal energy expenditure is still not fully enlightened.
It has been reported that energy consumed during resting period on subjects whom Roux-N-Y Gastric Bypass increased by 31%. Furthermore, among two subject groups who have same calories, the group who have not undergone Roux-N-Y Gastric Bypass has lost less weight by almost half (47%).
Roux-N-Y Gastric Bypass operation creates more efficient and permanent mechanisms which can not be explained by restriction of meals eaten or lack of absorption of some food. Patients has less eating desire emotionally after Roux-N-Y Gastric Bypass operation and a fullness and balance status are reached in whole body metabolically.
The irresistible activation strength of obesity surgery which can not be compared with non-surgical treatments seems as a tip that new mechanisms are pending to be discovered.
What are risks of Roux-N-Y Gastric Bypass Operation?
Stomach and intestine operations have possibility to cause many problems. Standard Risks of Gastric Bypass Operations
- Vitamin and mineral deficiencies due to absorption decrease.
- Sometimes diarrhea due to shorter intestinal distance,
- Osteoporosis,
- Insufficient or excessive weight loss,
- Nausea- Vomiting,
- Anastomosis leakage,
- Abscess or wound infection,
- Bleeding,
- Deep vein thrombosis,
- Pulmonary embolism,
- Fistula,
- Gall bladder or bile duct stones
- Stenosis on anastomosis,
- Partial or complete intestinal obstructions due to intra-abdominal adhesions,
- Incisional herniation (herniation appeared on port sites)
Early Term Risks After the Operation
Pulmonary embolism is a risk which may be seen in all operations of individuals with morbid obesity. It is seen in 1 to 2% of laparoscopic Roux-N-Y Gastric Bypass operations. It is caused by deep vein thrombosis. A clog separated from leg veins may obstruct lung vessels. We inject anti-coagulants (low molecular weight heparins) before laparoscopic Roux-N-Y gastric Bypass operation and during hospitalization period. We mobilise the patient at the day of surgery. However, these treatments do not guarantee that lung embolism will be prevented.
Leaks may be detected from transection and anastomosis stapler lines performed in the operation. These leaks are seen in 1 to 2% of laparoscopic Roux-N-Y Gastric Bypass operations. It is difficult to diagnose early. Obesity is an inflammatory case by itself. Furthermore, excesive fats in and around abdomen prevents to notice inflammatory response during early period. Early term palpitation or dyspnea are important for us. Restlessness after the operation may depend on an early leakage. It is useful to share the simplest negativity that you feel with your doctor at earliest time.
Some teams use specific materials to reduce these leakages. Some teams control if there is any leakage with radiological examinations performed with contrast medium x-rays. None of these are safe by 100%. Leakage may appear in Laparoscopic Roux-N-Y Gastric Bypass although specific materials are used. Or, it may not be seen in films although there is a leakage. Clinical monitoring of your surgeon is the most important factor.
Bleeding from operation site, wound infections, intestinal obstructions which may occur within several weeks are rare surgical complications which may appear after laparoscopic Roux-N-Y Gastric Bypass operation.
Long Term Risks After the Operation
Herniations are seen as most common on port sites during postoperative period following Laparoscopic Roux-N-Y Gastric Bypass operation. It is seen most common on the port site close to the umbilicus. This possibility is reduced by suturing the abdominal muscles at port sites over 10 mm where ports are placed after the surgery. Patches may also be placed into these port sites after the operation. This may increase economic costs.
Gallbladder stones may be detected by 3 to 30% after laparoscopic Roux-N-Y Gastric Bypass operation. The possible cause is considered that cholecystokinin hormone secreted from duodenum decreases after the surgery. Therefore, your doctor may suggest you removal of gallbladder during the surgery.
Mild nausea and vomiting are not complications. However, resistant and long term vomiting reminds a stenosis on the new connection (anastomosis) between your stomach and small intestine. This condition is called anastomotic stenosis. The patient is hospitalized and intravenous nutrition is planned. Extent of the stenosis is evaluated by radiological examinations performed with contrast medium. If one month has passed from the operation, endoscopic evaluation is performed. Endoscopy may provide opportunity for balloon dilatation of this stenosis. The problem can be resolved in most cases. If special sheats have been used to strengthen the stapler line while performing anastomosis, endoscopic dilatation is not preferred. Reconstruction is required by operation in this case.
Ulcer on anastomosis line may be detected by 3 to 10% after laparoscopic Roux-N-Y Gastric Bypass. These ulcers are seen more in small intestine part of the anastomosis because they generally depend on gastric acid. It regresses by drug therapy if it has not injured anastomosis line. Reconstruction with surgery may be necessary if anastomosis has been damaged.
Metabolic Side Effects
Dumping Syndrome:
Like all bypass operations, excess liquid diffuses into the intestines when voliminous carbohydrate is consumed. So much liquid in the stomach and jejunum causes bloating and tension in the lumen. Vascular fluid decreases because of fluid transit into the intestine and blood pressure decreases. Severe nausea and vomiting and syncope accompanies to this phenomenon.
Starchy foods should be avoided to prevent Dumping Syndrome. Foods including white flour and starch should not be consumed. White bread, pita and thin bread, pasta and bakery products are included in this group. Creams and creamy coffees may cause dumping syndrome if they are consumed much.
Dumping Syndrome is not a problem actually. Because this disturbing condition which appears with intake of foods including high calories is actually the mechanism of action of Roux-N-Y Gastric Bypass operation. Otherwise, strong and long term weight loss will not be possible.
Junk food eating habit which generally exists in most of individuals with morbid obesity is responsible from weight regaining after operations which reduce gastric volume only such as gastric band or gastric tube. Foods including high calories but in liquid or soft form are easily tolerated after volume restricting operations and they cause severe weight gain. In fact, Dumping Syndrome appeared after Roux-N-Y Gastric Bypass forces patients to give up this habit.
- Deficiency of iron, B12 and Folic acid appears after laparoscopic Roux-N-Y Gastric Bypass operation. Deficiency of these cause anemia. These are replaced with normal daily tablets. Intravascular or intramuscular injections may be necessary in very rare cases.
- Fat absorption mildly decreases after laparoscopic Roux-N-Y Gastric Bypass operation. Its assumed that vitamins absorbed in fats will have limited absorption. Vitamins A, D, E, K may be supplemented easily and sufficiently with daily vitamin tablets. Defecation may become softer and slightly malodor because of decrease on absorption. This odor disappears when fat ratio decreases in diet. However these effects of RYGB are mostly not seen. Because RYGB only bypasses the 5 % of all intestines and great majority of patients do not need life time supplementations. Only iron and B12 deficiency might be present and annual parenteral replacement easily covers the deficit.
The most efficient and permanent treatment of obesity is obesity surgery. Laparoscopic Roux-N-Y Gastric Bypass is the most common obesity surgery technique applied worldwide. If you can not loose weight with diets and other treatments that you tried, Roux-N-Y Gastric Bypass may be an appropriate treatment for you. If you loose and regain weight frequently, this may cause metabolic inefficiency and appearance of other diseases. Roux-N-Y Gastric Bypass may eliminate this condition.
